
 English
English  Português
Português  Español
Español by Alberto J. Muniagurria and Eduardo Baravalle
The abdominal surface can be topographically divided into nine regions by means of two horizontal lines, one at the level of the lower costal margin and the other at the level of the anterior superior iliac spines, and two vertical at the level of the middle of the femoral arch (Figure 10-1 ). Each topographic region will represent the location of different organs of the abdominal cavity. In a simpler way, it can also be divided into four regions or quadrants, two upper right and left, and two lower, also right and left (Figure 10-2).
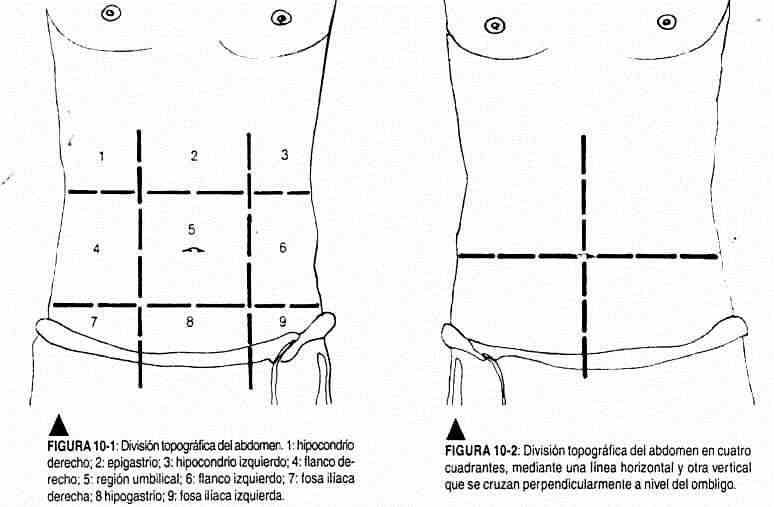
The right upper quadrant is the projection area of the liver, gallbladder, and duodenum, while the stomach, left lobe of the liver, and pancreas project into the epigastrium. The left hypochondrium corresponds to the stomach and the arm; in the umbilical zone the small intestine; on the right flank the ascending colon and the right kidney; on the left flank the descending colon and the left kidney; in the iliac fossae, the cecum on the right and the sigmoid on the left. In the hypogastrium the bladder and uterus project.
The physical examination of the abdomen begins with inspection, continues with auscultation, ending with percussion and palpation. The patient should be in the supine position, with his muscles relaxed, his head resting on a flat pillow and with the upper and lower limbs resting on the examination table. The patient should breathe calmly, with his genitals covered and the bladder empty. The light must be perpendicular and a tangential light will be used when it is considered necessary to highlight a beat or a movement through the play of shadows that is produced in this way. The temperature of the room will be adequate to avoid muscle contraction. The examiner's position can be standing or sitting; usually to the right of the patient, although on certain occasions, for the examination of the left upper quadrant, it will be convenient to stand to the left of the patient. An adequate temperature of the examiner's hands is important to avoid contraction of the muscles of the abdominal wall; This is achieved by rubbing the hands or placing them in hot water. It is advisable to wash your hands before beginning any semiological maneuver. It is common for the student or beginner to have cold and shaky hands, which reduces the quality of the information collected. The approach to the patient should be with slow and smooth movements and gestures, distracting attention if necessary with the conversation. He should be asked to collaborate through respiratory movements, the Valsalva maneuver, etc., with a firm and soft voice.
Inspection
The shape, the color of the skin, the state of nutrition, the presence of hair, the characteristics of the navel, the respiratory movements, the presence of normal heartbeats or fetal movements should be observed.
Once the abdomen has been inspected, the patient is asked to make an effort to distend it and another to retract it, carefully following the signs that become apparent. The anterior rectus muscles are clearly visible when the patient elevates the head.
The normal adult abdomen should not extend beyond an imaginary line connecting the xiphoid process with the pubis. In the child, the abdomen tends to be more globular and rounded; while in the elderly, adipose tissue accumulates in the lower areas, with looseness of the wall muscles. If there are abnormalities, the patient should be examined in the standing position. The umbilicus consists of a ridge and an umbilical groove, and under normal conditions it is seen as a depression that should not protrude with standing or with Valsalva maneuvers.
Auscultation
In the abdomen, auscultation precedes percussion and palpation, so that the sounds heard are spontaneous from the patient, and not those induced by percussion or palpation of the abdominal viscera. This maneuver has real utility in the presence of pathology.
The membrane of the stethoscope must be pre-warmed with the palm of the hand. Bowel sounds are transmitted well in the abdominal cavity, making it unnecessary to auscultate more than two areas.
Normal bowel sounds are high-pitched and originate almost entirely in the small intestine. They have gurgling characteristics (glu-glu), with a frequency of 5 to 30 per minute. Rumbling sounds are prolonged gurgling heard when peristalsis is increased. They are difficult to describe, but are easily identifiable once they have been heard. In some patients it is possible to auscultate murmurs in the epigastrium, which are meaningless and of unknown cause.
Palpation
Fingernails should be trimmed and hands clean, and warmed up before starting palpation. Starting palpation with cold hands can lead to rejection, contraction of the anterior wall musculature, and little collaboration on the part of the patient.
If tickling is aroused during these maneuvers, the patient should be discussed and distracted, maintaining a serious and professional attitude.
Deep palpation . Deep palpation is performed through the palmar surface of the fingers that deepen into the abdomen, at the level of the upper and lower right and left quadrants.
Superficial palpation . This palpation is performed with movements of the hand on the abdominal surface, with gentle flexion of the metacarpophalangeal joints (groping) or sliding of the exploring fingers over an area of the abdomen (tracking). These maneuvers help to relax the patient; its duration in the normal abdomen is short and precedes deep palpation. Relaxation of the muscles should be felt during exhalation.
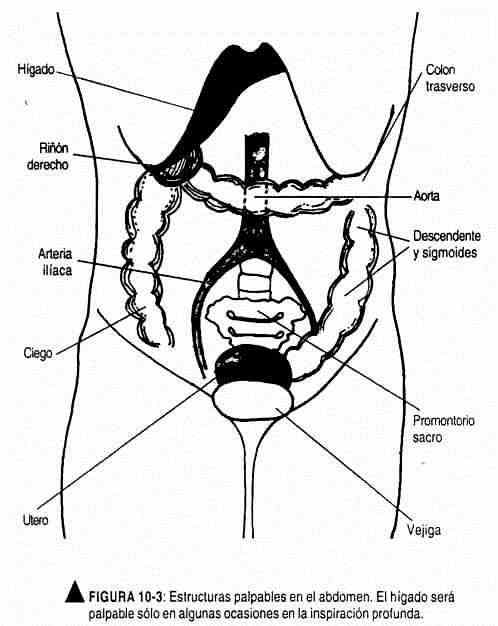
There are a number of structures and organs that can occasionally be palpated (Figure 10-3).
The liver, which is normally covered by the rib cage, can sometimes be felt during deep inspiration. The edge is firm, regular, and smooth, sometimes felt only as resistance.
The lower pole of the right kidney can be palpated in normal subjects, with thin and relaxed abdomens.
With the hands juxtaposed, the sigmoid colon can also be palpated under normal conditions in the left iliac fossa, recognizing it as a tube that rolls under the fingers of the examiner; sometimes this palpation can arouse slight discomfort in the patient. In the right iliac fossa, the cecum can usually be palpated with juxtaposed hands, causing slight pain. In healthy, lean subjects, the promontory of the sacrum, which is stony in consistency, is occasionally palpable. In the hypogastrium, the distended bladder and the gravid uterus can be palpated. The abdominal aorta can usually be palpated in the upper quadrants; in the lower ones you can feel the iliac pulses.
 Maneuvers for palpation of the liver . The liver is usually below the rib cage and is therefore not palpable. When it passes the bony border, as occurs in deep inspiration, either because the liver is enlarged or lowered, it can be palpated. The liver has wide respiratory mobility, with an edge that is blunt or sharp.
Maneuvers for palpation of the liver . The liver is usually below the rib cage and is therefore not palpable. When it passes the bony border, as occurs in deep inspiration, either because the liver is enlarged or lowered, it can be palpated. The liver has wide respiratory mobility, with an edge that is blunt or sharp.
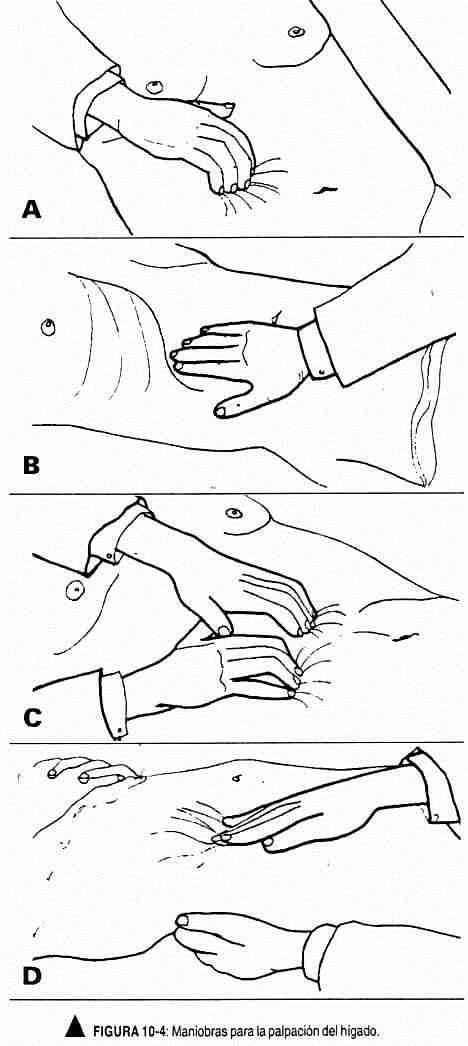
There are various maneuvers to palpate the liver, which is a deep palpation maneuver. It is convenient to be familiar with one of them. The patient, in the supine position, should breathe calmly, and when the examining hand is supported, they are asked to breathe deeply. The explorer hand (s) begin to palpate the right iliac fossa, taking advantage of each expiration to go up. They can be placed in various positions: the right hand "spooned" on the ulnar edge (Figure 10-4, A), with the fingers together and semi-flexed that will try to catch or perceive the lower edge of the liver at the moment of inspiration.
It can also be palpated with the examiner's right hand, located in a line parallel to the hemiclavicular line (Figure 10-4, B), who will perceive with the balls of the fingers the lower edge of the liver, which is felt as a bump. The bimanual maneuver, with hands juxtaposed, "hooked," and the examiner looking toward the patient's feet (Figure 10-4, C), will attempt to palpate the lower edge of the liver with each patient inspiration.
There is another very useful two-hand maneuver. The left hand is placed behind the patient, parallel to the eleventh and tenth ribs and pushing upward; the right hand, with the fingers to the side of the rectus anterior and pointing to the patient's head or in a discreet oblique position, begins palpation of the liver from the right iliac fossa (Figure 10-4, D).
Maneuvers for palpation of the spleen . In normal conditions the spleen is not palpable. Palpation of the spleen is a superficial palpation and can be performed from the right or the left of the patient. If it is palpable, a pole may be found that may have a notch and not an edge, with its long axis directed towards the umbilical area. It has respiratory mobility. With the examiner to the right of the patient (Figure 10-5, A), the left hand rests on the lumbar region and draws the left upper quadrant toward the examiner's right hand. This last hand, located obliquely, advances from the navel towards the eleventh and twelfth ribs with each expiratory movement. To perform this maneuver, the patient is asked to breathe deeply.
With the scanner to the left of the patient, one-hand or two-hand maneuvers can be performed. The left hand on the spoon, gently palpating, will advance from the navel towards the ribs, taking advantage of each expiration. At the end of the deep inspiration, he will attempt to palpate the spleen (Figure 10-5, B). This maneuver can be improved by resting the right hand on the patient's left hypochondrium and pressing said area; the left hand is the palpatory hand.
The spleen can also be palpated with the patient in the right lateral decubitus position, with the left knee flexed (Figure 10-5, C).
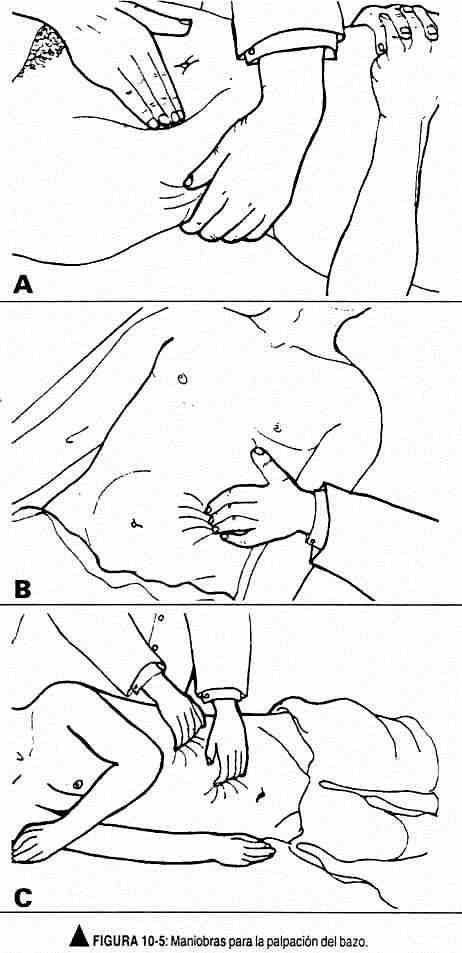
This position would facilitate the descent of an enlarged spleen. Then proceed as in the two previous maneuvers. Palpation of the spleen will be completed with percussion maneuvers, in order to establish the contour of the organ.
Maneuvers for palpation of the kidneys . The maneuver for palpation of the kidneys is a deep, bimanual maneuver that takes advantage of each deep exhalation to deepen the exploring hand. The kidney has lumbar contact, which allows it an anteroposterior mobility that is known as lumbar ball. Respiratory mobility is less than that of the liver, a characteristic for which it can be held with the exploring hands in the position it takes on deep inspiration. In addition, it is sensitive to the touch.
The examiner is positioned to the right of the patient to palpate the right and left kidney. The left kidney can also be palpated from the left of the patient.
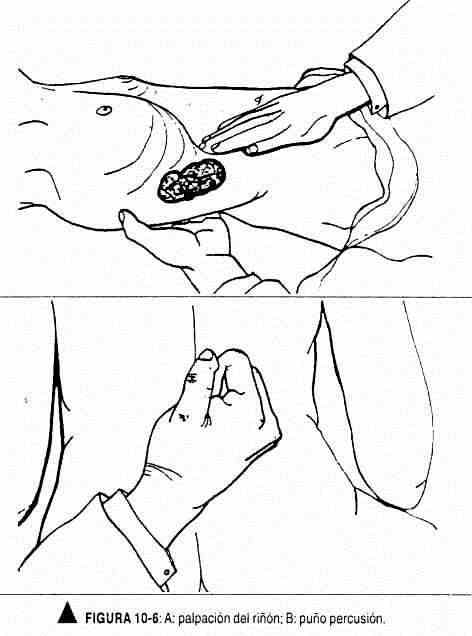
To palpate the right kidney or the left kidney from the right side, the left hand is placed in the lumbar area, with the balls resting on the mass of paravertebral muscles, the radial border on the lower border of the ribs and the ulnar border on the iliac crest. The right hand is located parallel to the anterior rectus muscle, or slightly oblique. At the peak of inspiration they are pressed. both hands, exerting more pressure with the front hand. As the patient begins to exhale, they are asked to stop exhaling, lower pressure is applied with the front hand, and the kidney is felt to slide upward, if it has been captured (Figure 10-6, A). To palpate the left kidney from the left side, the same maneuver is performed but in reverse.
Maneuvers for palpation of the aorta . The aorta is often palpated in the epigastrium. It is painful and the most important semiological characteristic is its heartbeat. To palpate it, press on the epigastrium, directly to the left of the midline. If the abdominal wall is thick, palpation should be bimanual, with each hand resting on the lateral wall of the aorta. In the case of thin abdomens, the aorta can also be palpated between the thumb and forefinger of the right hand.
 Percussion
Percussion
Percussion is a useful maneuver in the physical examination of the abdomen. It is used alternately and at the same time as palpation, to determine the size of the organs, generally the liver and spleen, identify air in the stomach or abdominal cavity, and rule out the presence of fluid or ascites in the abdominal cavity .
The presence of air in the stomach produces a high-pitched sound on percussion, called bloating. The sound produced by the percussion of adipose tissue and viscera such as the liver and spleen is called dullness.
The percussion should be smooth, with a reasonable amount of time between each beat, to prevent the sound of the subsequent beat from drowning out that of the previous beat.
Percussion of the liver is performed along the hemiclavicular line (Figure 10-7); It begins in the third intercostal space and descends space by space. At first the sound will be loud due to the characteristics of the pulmonary parenchyma, when reaching the fourth-fifth intercostal space a submatt sound will be obtained due to the interposition of the lung on the upper edge of the liver. Later the sound will be matte. This dullness should not extend down the costal margin, where the sound will be tympanic. Liver dullness should not exceed 10 cm in height, at the level of the hemiclavicular line.
The spleen percussion should be a gentle percussion. With the patient in the right lateral decubitus, it is started on the mid axillary line, where a sound is obtained due to the presence of lung tissue. The splenic dullness is at the level of the ninth and tenth costal arches, and does not exceed the eleventh costal arch; at the level of the tenth costal arch it must not exceed the mid-axillary line.
Gastric air bloat should be sought in the left upper quadrant (Figure 10-8). The lumbar fossa will also be percussed with the ulnar surface of the right fist closed (Figure 10-6, B). Normally the patient feels the blow, but without painful sensation.
