
 English
English  Português
Português  Español
Español by Alberto J. Muniagurria and Eduardo Baravalle
The general practitioner must always bear in mind that, when taking a patient's medical history, there is the possibility of finding a malignant disease. The reason for consultation can be varied:
- A periodic health check, focused on certain areas of the body; examples of this are the gynecological examination or the prostate examination.
-
It is a manifestation that leads directly to a malignant disease.
Examples of these are those listed by the American Cancer Society: prolonged fever of unknown origin; change in bowel habits; wounds that do not heal; changes in size or presence of nodules in the breasts and other organs or tissues; indigestion or trouble swallowing; changes in skin moles; cough or hoarseness - There are also signs and symptoms that do not directly show the presence of cancer, but that show, from the experience gathered, a significant percentage of association with malignant processes. For example, depression and the occurrence of phlebitis in pancreatic cancer, family history in colon and breast cancer.
- Likewise, there are patients who attend the consultation to assess the extent of a neoplastic disease.
Early detection is the biggest advance that has been made in recent decades. And in this sense, the exploration of symptoms and signs, the evaluation of hereditary antecedents, exposure to environmental predisposing factors, etc. are important.
 This chapter has organized the regional physical examination in search of neoplastic lesions. A thorough physical exam helps detect early breast cancer, cancer of the skin, head and neck, and colon. The order and method must be followed in a systematic way.
This chapter has organized the regional physical examination in search of neoplastic lesions. A thorough physical exam helps detect early breast cancer, cancer of the skin, head and neck, and colon. The order and method must be followed in a systematic way.
Attention should be directed to any painless, raised, irregular, hard lesion with firm edges, bleeding, or the presence of erythema, leukoplakia, or swelling.
Face . On examination of the face, asymmetries or swelling, ulcers or lesions with altered pigmentation may appear. The lips and mouth should be inspected and palpated in detail, helping each other to carry out the maneuvers with the index finger and thumb of the observer's right hand. The tongue depressor is useful to move the lips and improve the vision of the area.
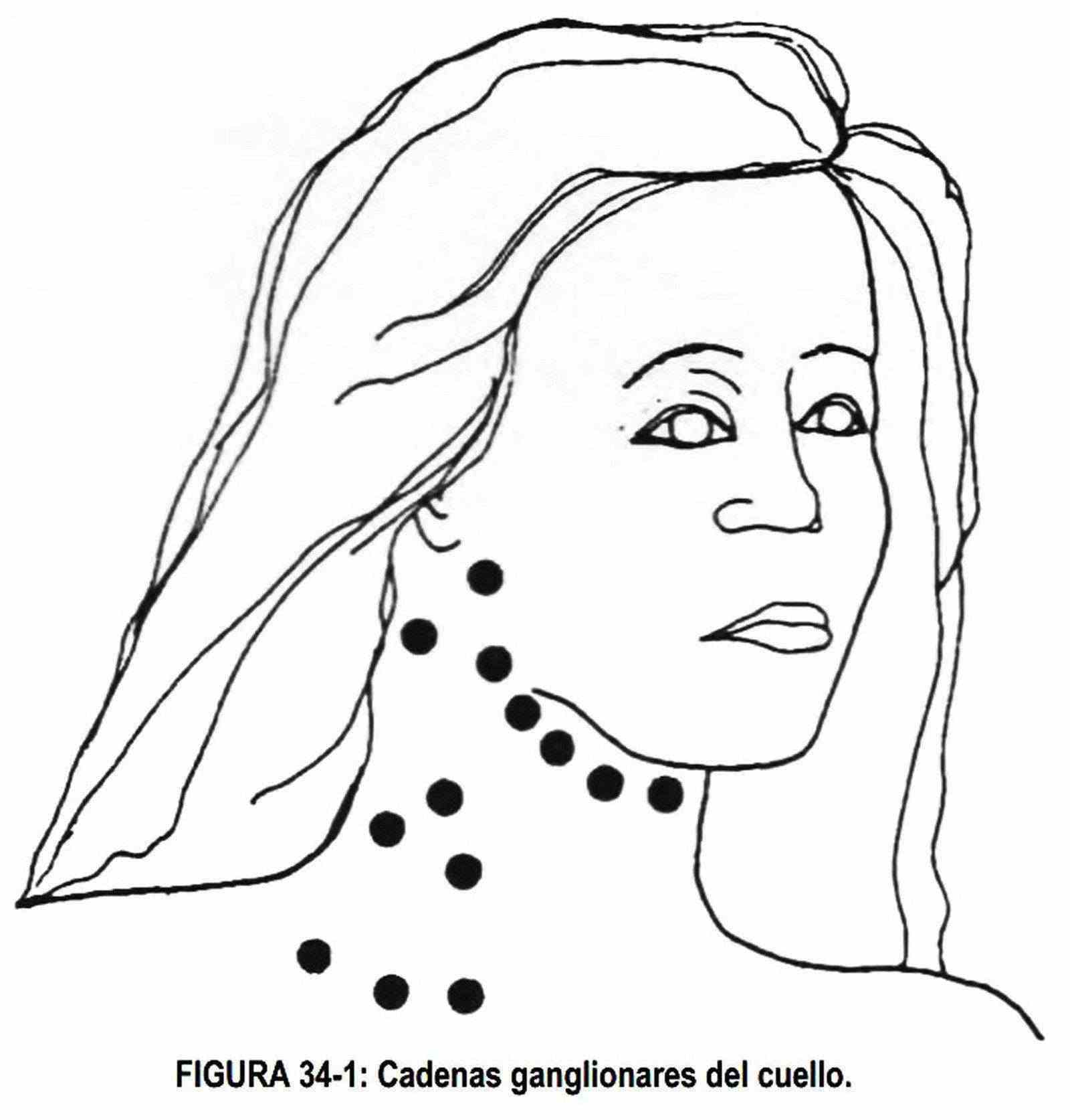
 Neck . Bimanual palpation of the neck should be performed for lymphadenopathy following normal anatomic chains (Figure 34-1).
Neck . Bimanual palpation of the neck should be performed for lymphadenopathy following normal anatomic chains (Figure 34-1).
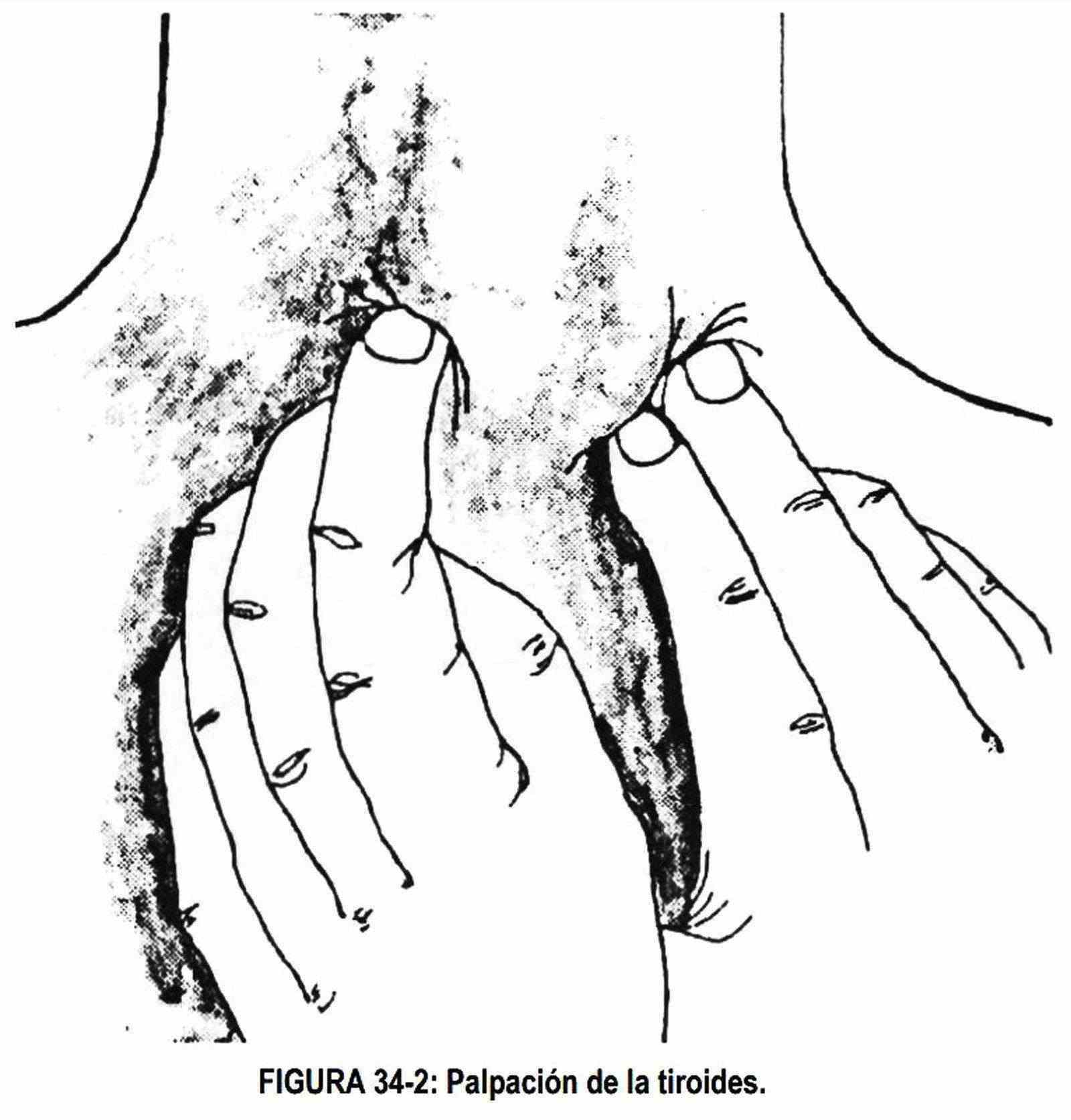
The parotic gland and submaxillary areas, as well as the pharynx and thyroid, will also be palpated (Figure 34-2). The thyroid must be palpated in its entirety; If a nodule is palpated, it must be described in terms of its location, shape and size, limits, consistency, relationship with other planes, existence of adenopathies, etc.
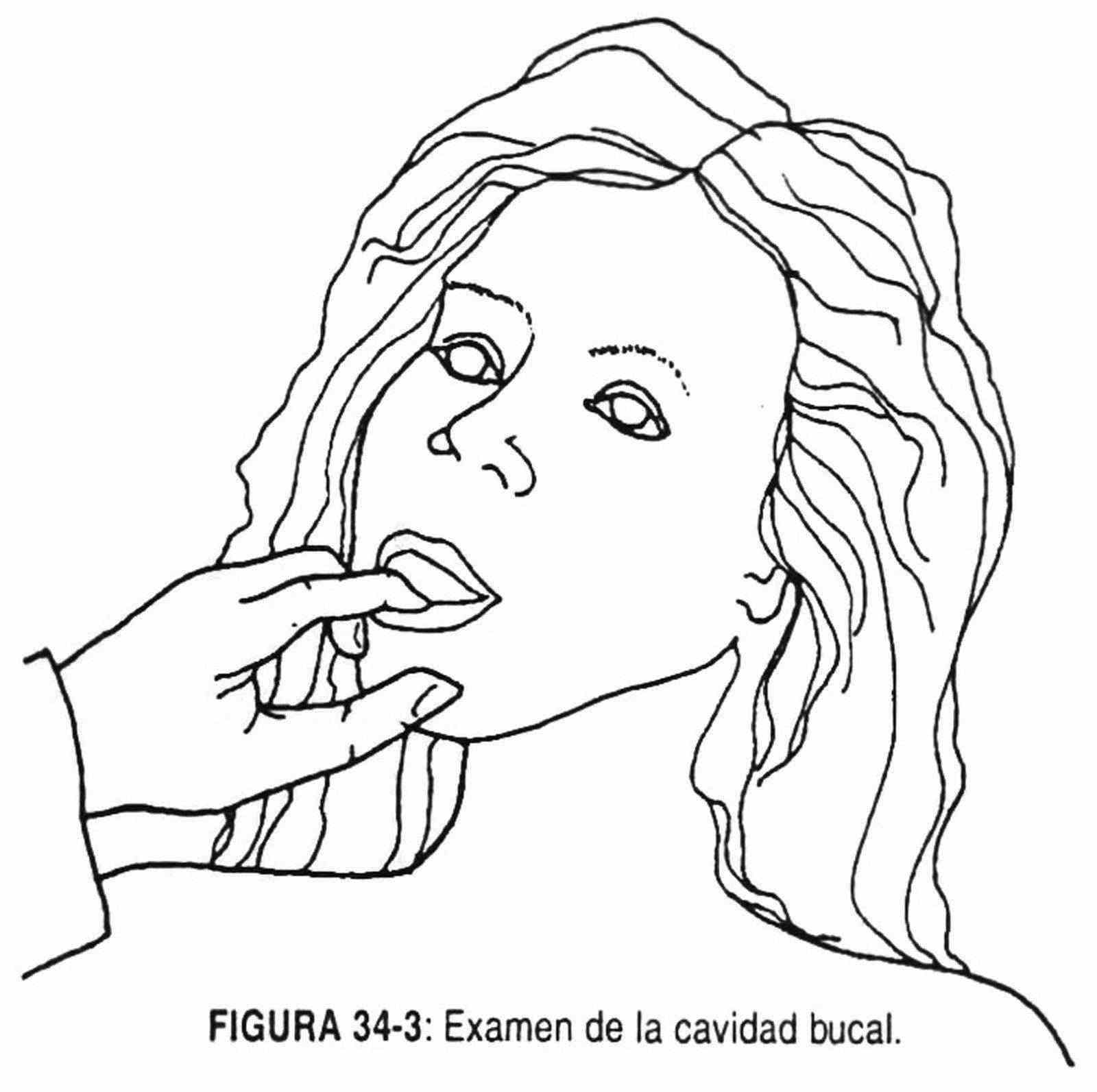
Mouth . Seventy-five percent of head and neck cancers begin in the oral cavity, so examination of this area should be thorough (Figure 34-3). The soft and hard palate will be inspected for hard or erythematous areas. Observe the gums, separating the cheeks with the observer's fingers. The tongue should be grasped with gauze and mobilized to facilitate inspection.
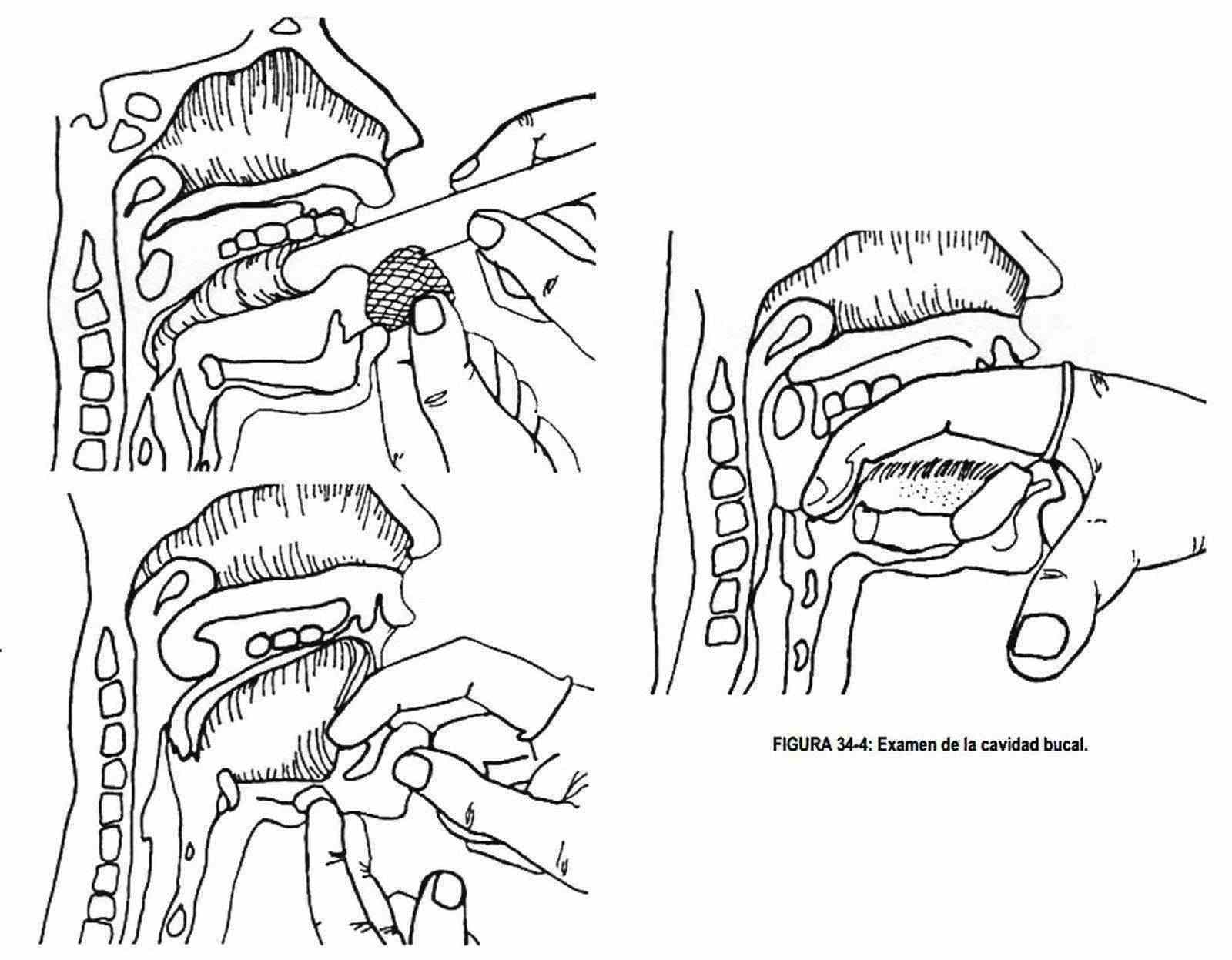
The floor of the mouth is still palpated between the tongue and the teeth with the gloved right hand (Figure 34-4).
The patient is asked to "stick his tongue out" and mobilize it. The base of the tongue is then palpated with the gloved hand in search of lumps, indurations, etc.
 Pharyngotonsillar area . With a small mirror with a handle, the pharyngeal area is observed, without touching the soft palate and pressing the tongue with the handle to fix the position.
Pharyngotonsillar area . With a small mirror with a handle, the pharyngeal area is observed, without touching the soft palate and pressing the tongue with the handle to fix the position.
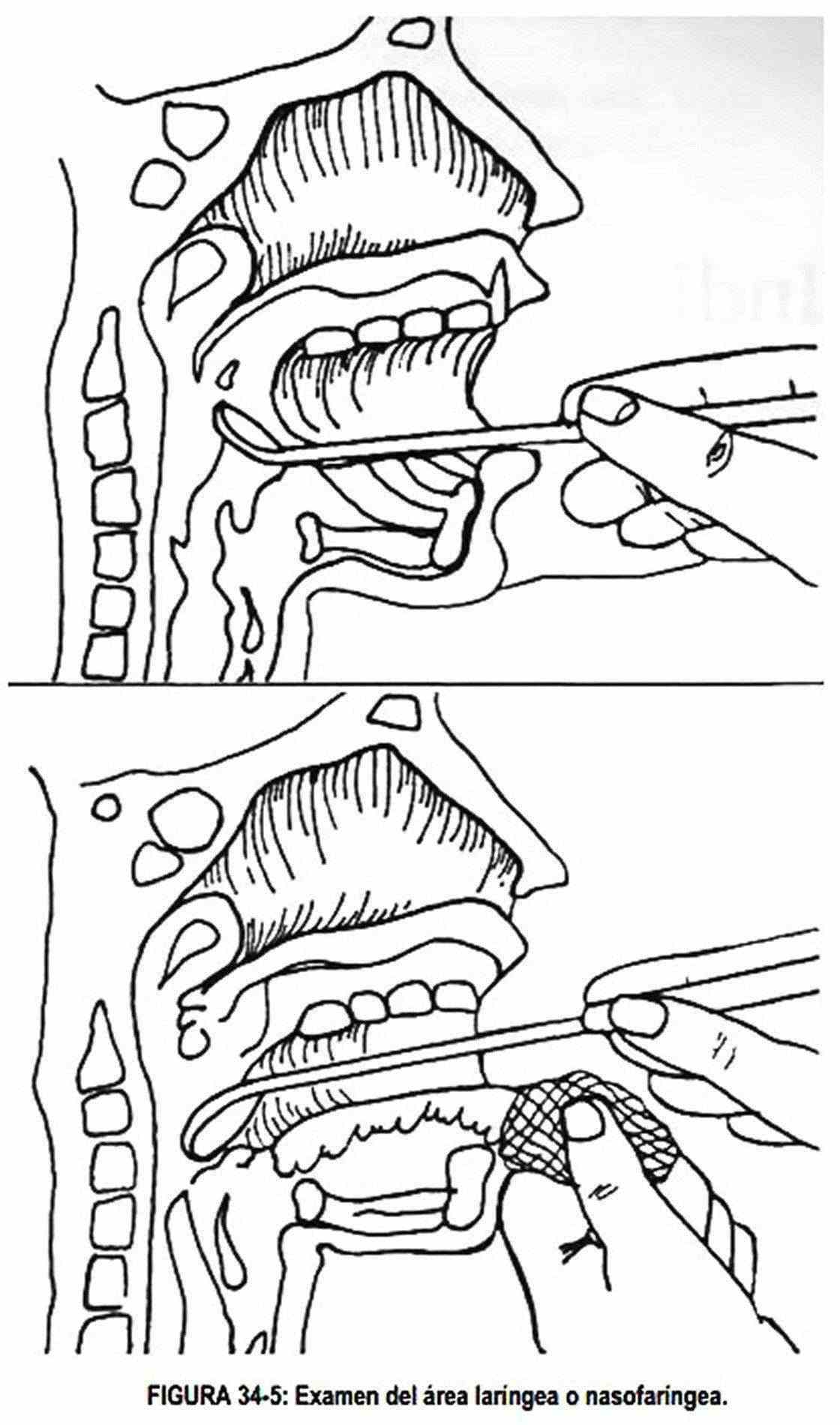
Laryngeal and nasopharyngeal area . Taking the tongue with gauze and holding the mirror in the right hand, the laryngeal and nasopharyngeal area is observed (Figure 34-5). To fix the mirror it must be supported on the tongue. The mirror must be pre-heated in a flame or hot water to avoid fogging. Check the temperature with the back of the hand before introducing it into the patient's mouth.
Skin . Examination of the entire skin surface should be thorough and detailed, paying special attention to areas that are not exposed to direct observation by the patient or any observer. The presence of depigmented or pigmented areas, especially in areas of friction, must be controlled. The inspection will be accompanied by palpation of the surface of the body with the hand in a flat way, looking for small lumps that would otherwise go unnoticed.
Mamas . The supraclavicular area, both breasts and nipples, and both armpits should be inspected and palpated. To perform this test, the patient will be in a sitting position and then lying down. After the examination is completed, the patient will be taught to perform her own breast evaluation. This self-examination should be done once a month. The best time to do it is when your breasts are soft, mobile and not engorged. During the habitual bath of the patient with the wet breast and with soap, the sensitivity is greater. You will be taught to look at the nipple, as well as to look for discharge.
Then you will continue your exam in supine position and with a small pillow under the shoulder corresponding to the examined breast. He should be taught to divide the breast into quadrants and to palpate it thoroughly by pressing it against the rib cage. If you notice anything out of the ordinary, you shouldn't be alarmed, but you should see your doctor. Lesions of the breast are described in the corresponding chapter.
 Routine gynecological exam . Examination of the external and internal genitalia, with smear cytology and bimanual palpation of the cervix, uterus and annexes should be performed periodically. When there is excessive flow, abnormal bleeding (metrorrhagia), intermenstrual, postmenopausal or postcoital losses, or water losses, before performing hormonal treatments it is necessary to perform a gynecological examination.
Routine gynecological exam . Examination of the external and internal genitalia, with smear cytology and bimanual palpation of the cervix, uterus and annexes should be performed periodically. When there is excessive flow, abnormal bleeding (metrorrhagia), intermenstrual, postmenopausal or postcoital losses, or water losses, before performing hormonal treatments it is necessary to perform a gynecological examination.
Bimanual palpation.With the index and middle fingers of the right hand, gloved and lubricated, the pelvic structures are palpated, noting their mobility, consistency, size, shape, neck limits, etc. If a mass is palpated, it must be defined semiologically. For greater comfort, the examiner should rest his elbow on his right knee, which will be elevated, since the right foot rests on a stool below the table. The abdomen is palpated with the left hand. To palpate the neck for symmetry and consistency, the uterus is compressed with the abdominal hand against the finger placed in the vagina. The uterus, in turn, is raised with the intravaginal hand to feel it with the abdominal hand. Cancer of the uterus may exist in a semiologically normal uterus,
The adnexa are palpated by directing the intravaginal finger toward the fornix and bringing the fingers of the abdominal hand toward the observer. The ovaries are tender to palpation.
Rectovaginal palpation . The index finger of the right hand, gloved and lubricated, is inserted into the vagina, and the middle finger with the same care into the rectum. Information is collected on the rectovaginal septum and the posterior aspect of the uterus. Towards the sides, data on the parametria is obtained.
Rectal exam. The rectal exam is a practice that should be performed once a year in every man over forty years of age.
It is also performed in all patients who consult for blood loss through their digestive tract, change in defecatory habits, pushing, tenesmus, etc. or pain. Positions to do so are described in Chapter 11.
First the inspection is carried out, searching when separating the buttocks, areas of depigmentation, scars and fistulas at the level of the anus. Undergarments will be checked for blood stains.
When separating the anal area with both hands, thrombosed or prolapsed hemorrhoids or prominent nodular lesions that characterize anal carcinoma can be seen.
Digital examination of the anus and rectum (digital rectal examination) . Using the gloved right hand, insert the lubricated index finger into the rectal opening. Look for the presence of masses and pain and evaluate the tonism of the anal sphincter. The patient should be asked to push the furthest areas closer to the finger. The posterior aspect of the rectum is, in general, an area that is poorly visualized on endoscopy, for which reason it is convenient to palpate. An examination of the prostate gland should also be carried out, describing its shape, size, consistency, limits, sensitivity and presence or absence of nodulations.
Bidigital examination . With the right index finger in the rectal orifice, the thumb of the same hand is placed on the tip of the coccyx. Then the hand will be progressively rotated palpating the entire anoperineal surface.
With these maneuvers the examining hand can feel or palpate a sessile or pedunculated adenoma or villous papillomas. The sessile adenoma is mobile, small, and firm; the pedunculate is more mobile and has a stem attached to the wall; villous papillomas, in turn, are granular and smooth. The cancer infiltrates, is hard, nodular and irregular. It has a fixed and ulcerated base and its size can vary from a small to a large lesion that occupies the entire circumference of the rectum. When removing the finger it is important to look for blood or mucous or mucopurulent material.
Leaving the index finger on the rectum, the described maneuver can be completed by palpating the abdomen with the right hand.
The examination should be completed with an anoscopy and a rectosigmoideoscopy, and if necessary with a colonofibroscopy.